Patient Guide · Knee Surgery
Your Meniscus Tear, Explained
The small piece of cartilage that protects your knee for life, and why what you do about a tear matters more than it feels like it should.
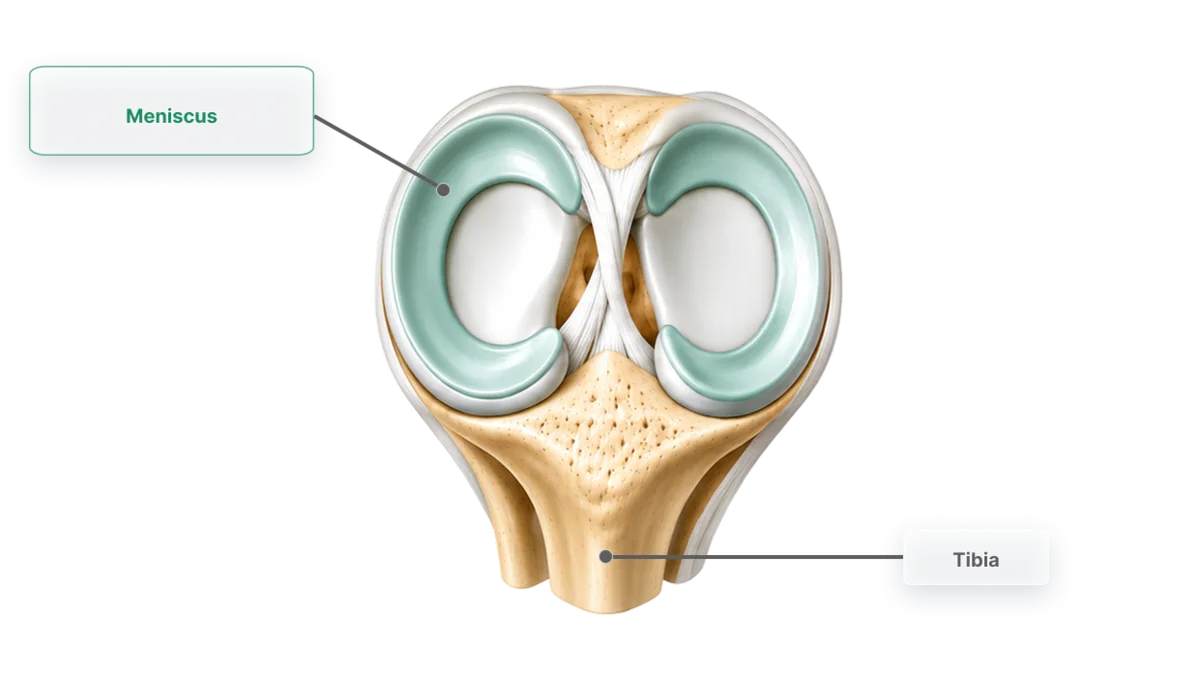
What the meniscus actually does
You have two menisci in each knee, tough, C-shaped wedges of cartilage that sit between your thigh bone and shin bone. Think of them as the knee's shock absorbers and load-spreaders: they turn a small point of contact into a broad cushion, so every step, squat and landing is shared across the joint instead of hammering one spot. They also add stability and help the joint glide smoothly. An intact meniscus is one of the single best protections you have against knee arthritis.
What happens when it tears
Meniscus tears happen two ways. In younger, active people they're usually an injury, a twist or deep squat with the foot planted, often alongside an ACL tear. In people over about 40 the cartilage gradually wears and can tear with something as ordinary as standing up from a low chair; these are called degenerative tears. Typical symptoms are pain along the joint line, swelling, and a knee that catches, clicks or feels like it's about to lock.
Not all meniscus tears are the same
The meniscus is a C-shaped cushion of cartilage that spreads load across the knee. When it tears, the pattern of the tear, its direction, size and where it sits, matters as much as the fact that it's torn. Two people can both have "a meniscus tear" and need completely different treatment.
Broadly, a surgeon is weighing one question: can this tear be repaired (stitched so it heals), or is the damaged part better trimmed away? Repairing preserves more of the natural cushion, which protects the knee over the long term, but it asks more of the recovery and doesn't always heal. Trimming gets you moving sooner, but removes tissue that can't be replaced. Neither is automatically "better"; it depends on the tear.
What a surgeon considers when deciding to repair or trim
The single biggest factor is blood supply. The meniscus is well supplied with blood only around its outer rim (often called the "red zone") and has almost none at its inner edge (the "white zone"). A tear in the outer rim has a real chance of healing if stitched; a tear at the inner edge usually won't heal no matter how it's treated, so trimming is often the more honest option.
Alongside that, a surgeon typically weighs the tear pattern (which direction it runs, and whether stitches can hold it), the size and stability of the tear, the quality of the tissue (healthy tissue repairs; frayed, worn tissue often doesn't), and your own circumstances: age, activity level, how recently it happened, and whether anything else in the knee is being treated at the same time (repairing a meniscus during an ACL reconstruction, for example, tends to heal better). The final decision is always made by your treating surgeon for your individual knee, and sometimes only once they can see the tear directly during surgery.
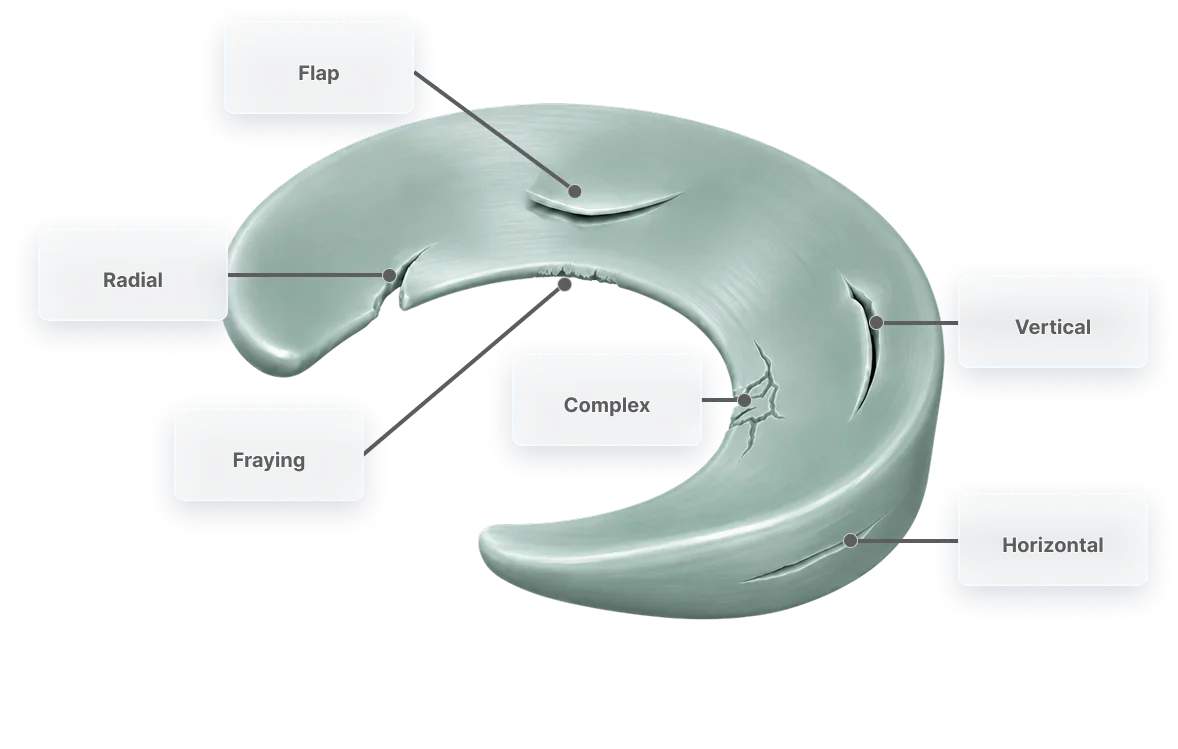
The main tear patterns
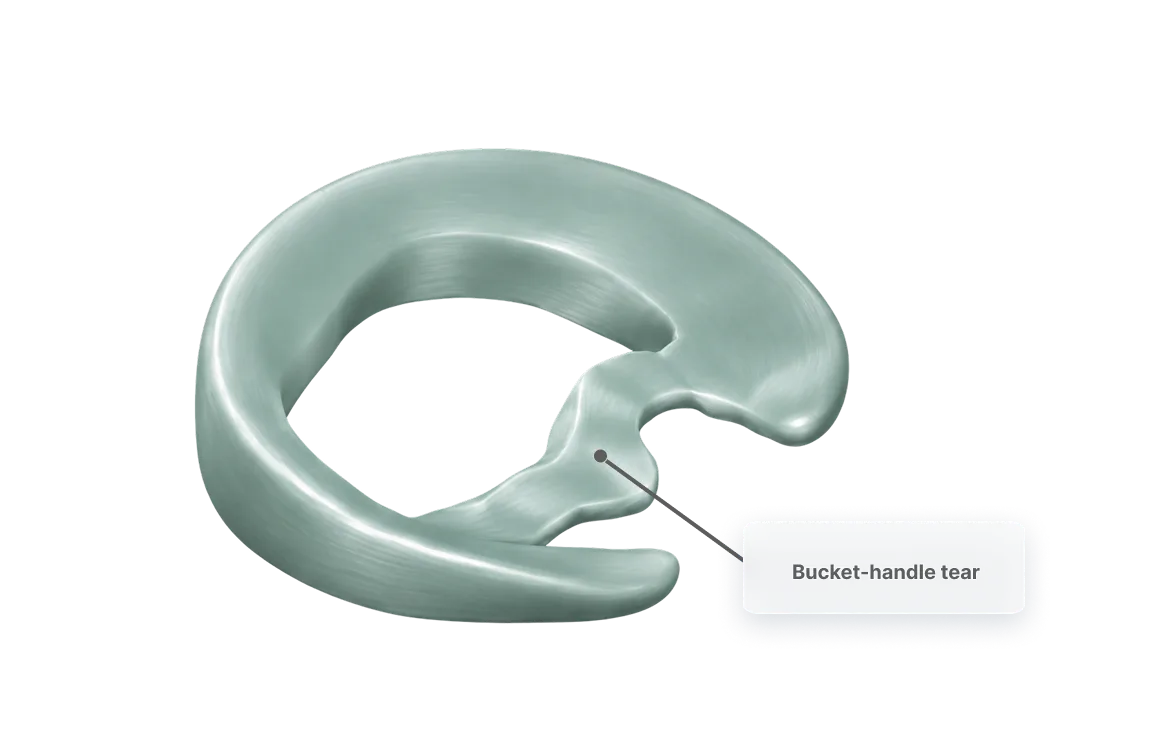
Bucket-handle tear
A large longitudinal tear where the loosened piece flips into the middle of the joint like a bucket handle; it can lock the knee or stop it fully straightening. Less common, but important: it's often treated as a priority, and in a younger knee with good tissue it is frequently repaired rather than removed.
Longitudinal (vertical) tear
Runs lengthwise along the cushion, in the same direction as its natural fibres. Common in younger, more active knees and often seen alongside an ACL injury. When it sits in the outer, blood-rich zone, this is the pattern most likely to be repairable.
Radial tear
Runs from the inner edge outward, cutting across the natural fibres. This is one of the more commonly seen patterns and can affect the cushion's function even when small. Whether it can be repaired depends heavily on how far out it reaches: those extending to the blood-rich rim may be repaired, while inner-edge radial tears are often trimmed.
Horizontal (cleavage) tear
Splits the cushion into upper and lower layers, like slicing through the middle. More common in middle-aged and older knees, where it's usually part of gradual wear rather than a single injury. Repair is selective, considered more often in younger patients, while worn, degenerative versions are frequently trimmed or managed without surgery.
Root tear
The cushion pulls away from its anchor point on the bone rather than tearing in its body. Historically under-recognised but increasingly diagnosed, because losing the anchor means the cushion can no longer do its job, so where the tissue is healthy, surgeons increasingly aim to reattach it rather than leave it.
Flap tear
A piece of the meniscus lifts and catches in the joint. Flap tears are common, and usually trimmed, because the loose flap rarely holds stitches.
Your treatment options, honestly
Not every meniscus tear needs surgery. Well2Wise will help you work out which path fits your knee, age, tear pattern and goals:
Rehabilitation and time
Many degenerative tears, and small stable tears, settle with structured physiotherapy, activity modification and time. For a lot of over-40 tears, good-quality rehab produces results as good as surgery, and it's the sensible first step. Well2Wise supports patients through this pathway.
Partial meniscectomy (trimming the tear)
When a tear can't be repaired, the surgeon arthroscopically trims away just the damaged, unstable fragment and preserves as much healthy meniscus as possible. It settles symptoms quickly and reliably, but every millimetre of meniscus removed is load-spreading you don't get back, which is why surgeons remove as little as they safely can.
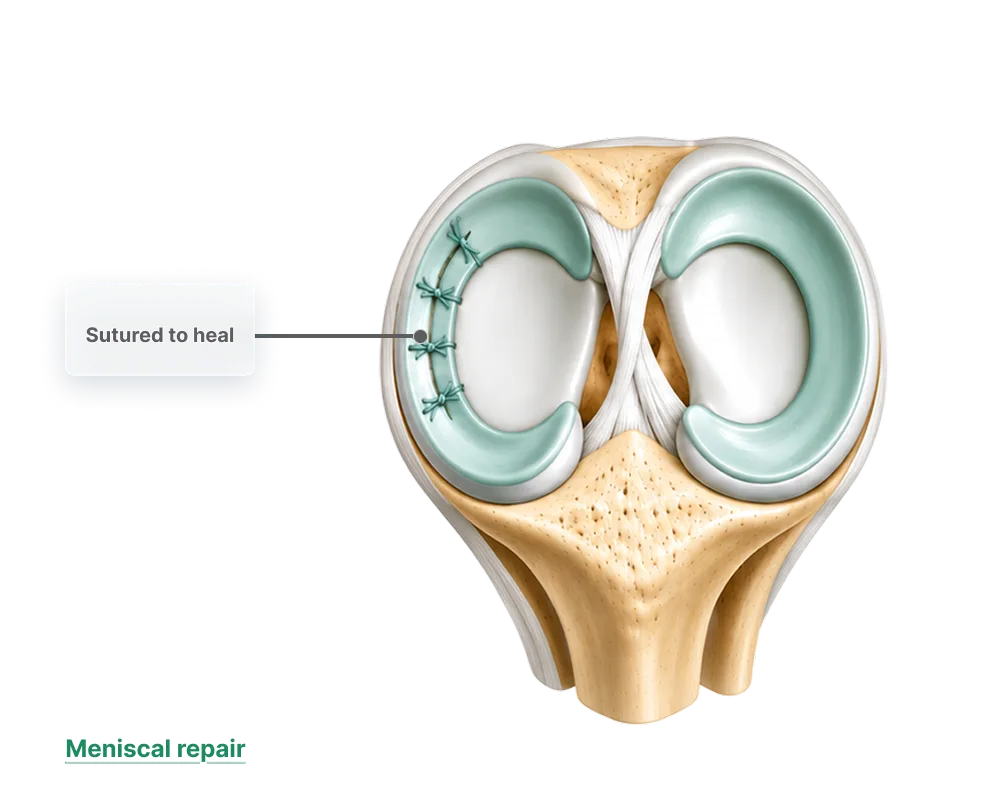
Meniscal repair (saving the meniscus)
When a tear is in the outer, blood-supplied zone, especially in younger patients, the surgeon stitches it back together so it can heal. It asks more of your recovery than a trim, but it preserves the cartilage that protects your knee for decades. Where a repair is possible, it's almost always worth it.

Thinking in decades, not months
The meniscus is a one-way asset: you're born with all of it you'll ever have. The right question isn't just "how do I feel better this month?" but "how do I keep the most cushioning in this knee for the next thirty years?" That's why, when a tear is repairable, saving it usually beats trimming it, and why a knee that keeps catching and swelling shouldn't just be ignored. Protecting your meniscus today is protecting yourself against arthritis tomorrow.
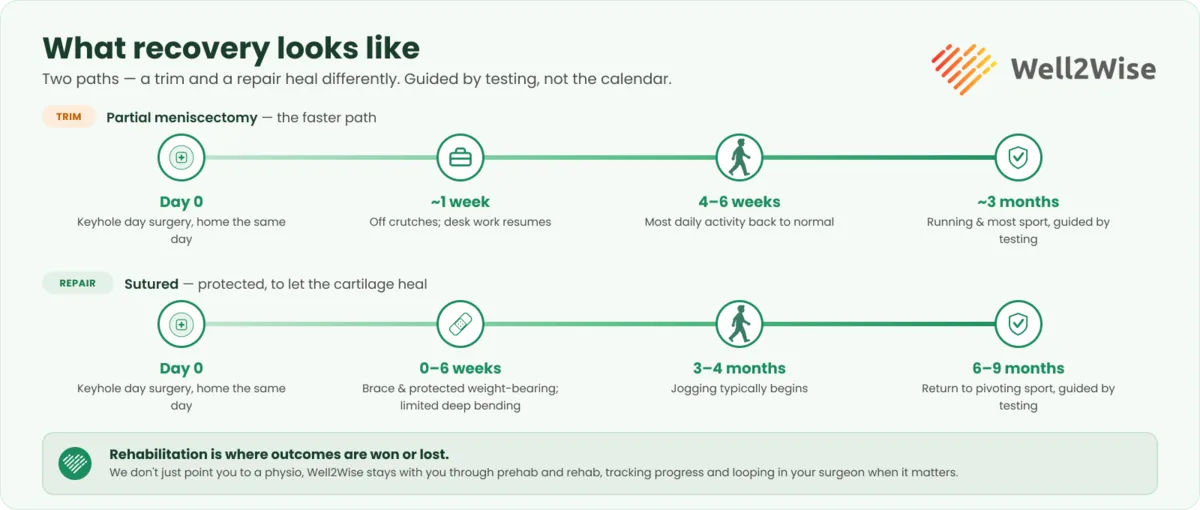
What surgery and recovery look like
Meniscus surgery is keyhole (arthroscopic) day surgery. Recovery depends heavily on which operation you had; a trim is quick, a repair is protected for longer to let the cartilage heal:
As with every knee operation, rehabilitation is where outcomes are won or lost, which is exactly why Well2Wise connects every surgical patient with a trusted physiotherapist for structured prehab and rehab as part of the pathway.
The Well2Wise pathway
Well2Wise is a booking and payment platform that connects you to care and coordinates it; the surgery itself is provided directly by your surgeon and an accredited Sydney private hospital.
Assess
A Rapid Physio telehealth triage, or book a surgeon consultation in the app for a personalised assessment (you'll need a current GP referral and MRI).
Prepare and recover
Well2Wise connects you with a trusted physiotherapist for prehab and rehab, with transparent pricing.
All-inclusive surgery when it's needed
Well2Wise connects you with a fellowship-trained orthopaedic knee surgeon, including surgeons who operate on elite footballers and other professional athletes, and coordinates one all-inclusive estimate covering surgeon, hospital, anaesthetist, implants, brace, medications and every post-op consult. No private health insurance required.
Your meniscus package depends on what your knee needs
Each is a single all-inclusive estimate. Your surgeon confirms which one fits your knee at your consultation, before you commit, and whether your tear is best repaired, trimmed or managed without surgery at all. The non-hospital components are fixed; the hospital component is confirmed directly by the hospital.
This guide is general information, not individual medical advice. Outcomes vary and all surgery carries risk. Discuss your situation with a qualified health practitioner. © 2026 Well2Wise Pty Ltd.
Not sure if your meniscus tear needs surgery?
Start with a Rapid Physio triage or book a surgeon consultation through the Well2Wise app, and get a clear, coordinated plan with transparent pricing.