Patient Guide · Knee Surgery
Your ACL Injury, Explained
And how to get it right the first time, a decision that shapes your knee for decades.
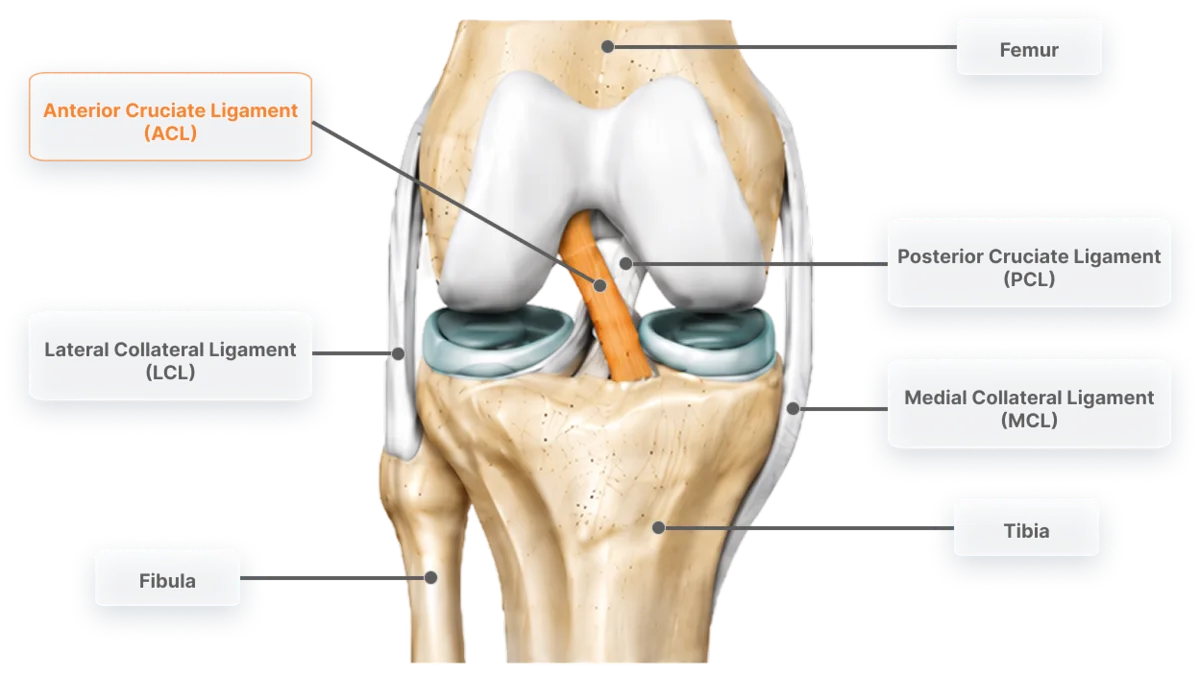
What the ACL actually does
The anterior cruciate ligament is the central pivot of your knee. It stops your shin bone sliding forward under your thigh bone and, more importantly for real life, it controls rotation every time you change direction, step off a kerb unexpectedly, turn to chase a toddler, or plant your foot on uneven ground. You don't just use your ACL for sport. You use your knee every single day, and the ACL is what makes it trustworthy.
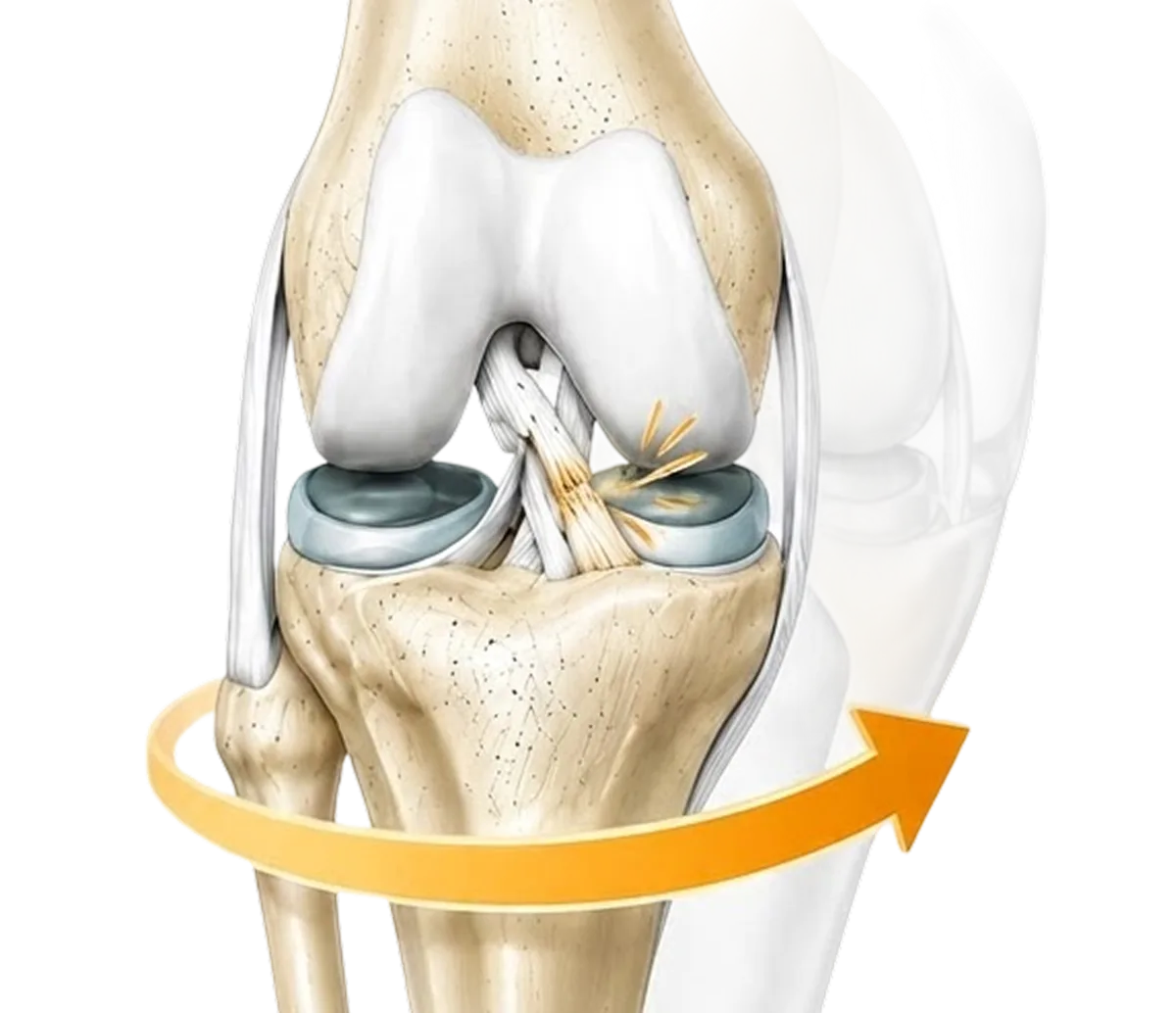
What happens when it ruptures
Most ACL ruptures happen without contact: a sudden change of direction, an awkward landing, a pivot with the foot planted. You may hear a pop, the knee swells within hours, and once the swelling settles the knee often feels almost normal, until it gives way. That giving-way episode is the ACL-deficient knee failing at its real job: rotational control.
Every giving-way episode risks new damage, most often to the menisci, the shock-absorbing cartilage pads that protect your knee against arthritis.
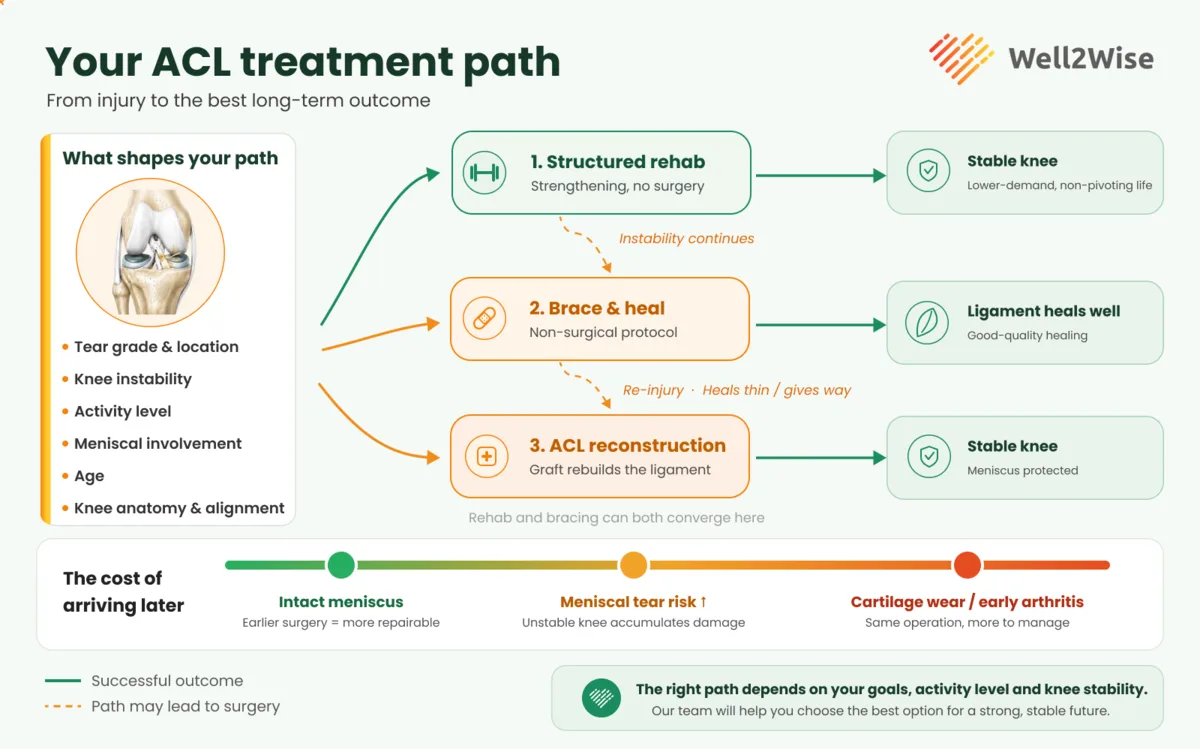
Your treatment options, honestly
There are three broad paths, and Well2Wise will help you work out which is right for your knee, age, sport and life.
First, what shapes your pathway
There's no single right answer for every knee. Your surgeon will review your MRI and examine your knee, then weigh these factors, broadly in the order they assess them, and talk them through with you before recommending a path:
- Tear grade & locationThe starting point: whether the ligament is partly or fully torn, and where, which shapes whether healing is even possible.
- Knee instabilityHow often the knee gives way, the leading indication for surgery and the single biggest driver of ongoing joint damage.
- Activity levelReturning to pivoting sport or physical work raises the demand on the knee, and the value of a stable, reconstructed one.
- Meniscal involvementA meniscus tear worth repairing raises the priority of surgery, and the urgency, since it's best saved early.
- AgeSkeletal maturity and biology set the context, younger, still-growing knees are approached differently to lower-demand ones.
- Knee anatomy & alignmentRefines the surgical plan: the natural slope and alignment of your bones can raise re-tear risk, so a graft-protecting step such as a lateral tenodesis (LEAT) may be added.
With that in mind, here are the three broad paths:
Structured rehabilitation alone
Some people, typically lower-demand, non-pivoting lifestyles, cope well without an ACL after high-quality rehab. This is a legitimate path, and Well2Wise supports patients through it.
Non-surgical "healing" protocols
You may have seen coverage suggesting a torn ACL can heal in a brace. There's genuinely interesting early research here, and important fine print most of the marketing leaves out. See our companion guide: Surgery vs Brace-and-Wait: The Questions to Ask.
ACL reconstruction
The torn ligament is replaced with a graft, performed arthroscopically by a fellowship-trained surgeon. The graft is usually your own tissue, an autograft, taken from your hamstring, patellar tendon or quadriceps tendon. In some cases it's an allograft: tissue from a screened, sterilised donor, which avoids taking tissue from your own leg but can heal more slowly and is generally reserved for specific situations such as revision surgery or older, lower-demand patients. For young, active people and anyone returning to pivoting sport or physical work, it's the most predictable way to restore a stable knee, and the only option that lets the surgeon repair meniscal damage at the same time.
Thinking in decades, not months
The right question isn't "how do I avoid surgery this year?" It's "what will this knee be like when I'm 45, 55, 65?" A knee that keeps giving way accumulates meniscal and cartilage damage that no operation can fully undo later. A well-reconstructed, well-rehabilitated knee with intact menisci is the best long-term asset you can give yourself. Surgery is a bigger upfront investment of time and money; instability is a loan against your future knee, with a punishing interest rate.
What surgery and recovery look like
Recovery is guided by testing and milestones, not the calendar:
Rehabilitation is where outcomes are won or lost, which is exactly why Well2Wise connects every surgical patient with a trusted physiotherapist for structured prehab and rehab as part of the pathway.

The Well2Wise pathway
Well2Wise is a booking and payment platform that connects you to care and coordinates it; the surgery itself is provided directly by your surgeon and an accredited Sydney private hospital.
Assess
A Rapid Physio telehealth triage, or book a surgeon consultation in the app for a personalised assessment (you'll need a current GP referral and MRI).
Prepare and recover
Well2Wise connects you with a trusted physiotherapist for prehab and rehab, with transparent pricing.
All-inclusive surgery when it's needed
Well2Wise connects you with a fellowship-trained orthopaedic knee surgeon, including surgeons who operate on elite footballers and other professional athletes, and coordinates one all-inclusive estimate covering surgeon, hospital, anaesthetist, implants, brace, medications and every post-op consult. No private health insurance required.
Your ACL package depends on what your knee needs
Each is a single all-inclusive estimate. Your surgeon confirms which one fits your knee at your consultation, before you commit. The non-hospital components are fixed; the hospital component is confirmed directly by the hospital.
This guide is general information, not individual medical advice. Outcomes vary and all surgery carries risk. Discuss your situation with a qualified health practitioner. © 2026 Well2Wise Pty Ltd.
Not sure which path is right for your knee?
Start with a Rapid Physio triage or book a surgeon consultation through the Well2Wise app, and get a clear, coordinated plan with transparent pricing.